
Zygote Intra-Fallopian Transfer (ZIFT) is an advanced assisted reproductive technology (ART) used to treat infertility in women. It is a fertility treatment that combines elements of both In Vitro Fertilization (IVF) and Intra-Fallopian Transfer (GIFT), designed to address certain infertility issues by placing fertilized eggs (zygotes) into the fallopian tubes for implantation, rather than the uterus.
The ZIFT procedure begins with egg retrieval and fertilization in the laboratory. The fertilized eggs (zygotes) are then placed directly into the woman’s fallopian tubes (rather than the uterus as in IVF). The fallopian tubes provide a natural environment for the zygotes to travel to the uterus and implant, where pregnancy can occur.
ZIFT is typically recommended when IVF alone may not be effective, particularly in cases where a woman has healthy fallopian tubes and is capable of conceiving naturally if the fertilized egg reaches the uterus. ZIFT allows the fertilized eggs to naturally travel through the fallopian tubes to the uterus, where they can implant more successfully.
The key benefit of ZIFT is the use of the fallopian tubes, which provide a more natural process for early embryo development. However, it requires that the woman have at least one functional fallopian tube.
ZIFT is often chosen when other fertility treatments, like IVF, have not been successful or when there are specific conditions that make this procedure more viable. The primary factors that make ZIFT a suitable option are based on fertility issues that affect egg fertilization, embryo development, or the embryo's journey to the uterus.
Blocked or Damaged Fallopian Tubes (when tubes are partially functional):
If a woman has partially blocked fallopian tubes but they are still capable of allowing the fertilized egg (zygote) to pass through, ZIFT may be a better option than IVF. The eggs are retrieved, fertilized, and then placed into the fallopian tube where they can travel to the uterus.
Infertility due to Ovulation Disorders:
Women with ovulation disorders (such as polycystic ovary syndrome (PCOS)) that cause irregular ovulation may benefit from ZIFT. The procedure ensures that a fertilized egg is placed in the fallopian tube, bypassing potential obstacles related to the uterine environment.
Male Infertility:
ZIFT can be used when male infertility, such as low sperm count or sperm motility issues, prevents sperm from successfully fertilizing the egg in a natural setting. The eggs can be fertilized in the lab, and ZIFT can help ensure they are placed in the fallopian tube for proper development and implantation.
Unexplained Infertility:
In cases of unexplained infertility, where no clear cause can be determined for the difficulty in conceiving, ZIFT may provide a better chance at success compared to IVF.
Failure of IVF:
ZIFT may be considered for women who have had failed IVF cycles. If the reason for IVF failure is unclear, or if embryos failed to implant in the uterus, ZIFT might offer a solution, allowing the embryo to be placed directly in the fallopian tube, where the conditions may be more favorable for embryo development.
Age:
Maternal age plays a significant role in fertility, and ZIFT is more commonly used for women under the age of 40 who have healthy fallopian tubes.
Previous Fertility Treatments:
If a woman has experienced multiple failed attempts with IVF, ZIFT may be suggested as a next step to improve the chances of successful pregnancy.
Tubal Issues:
Women with a history of tubal surgery, tubal ligation, or previous pelvic infections may have damage to their fallopian tubes that can affect fertilization and embryo transport. ZIFT can still be an option for those with partial tubal blockage or functional tubes.
ZIFT itself does not cause any specific symptoms, as it is a procedure rather than a condition. However, there are indicators and signs associated with the fertility issues that lead to ZIFT treatment. These are typically related to underlying infertility factors such as hormonal imbalances, reproductive tract issues, or egg quality.
Difficulty in Conception:
Couples who have been trying to conceive without success for 12 months or longer (or 6 months for women over 35) and who have been diagnosed with infertility may require ART procedures like ZIFT.
Irregular Menstrual Cycles:
Women with irregular menstrual cycles or ovulation problems often face difficulties with natural conception. In such cases, ZIFT may be used after egg retrieval and fertilization in the lab.
Blocked or Damaged Fallopian Tubes:
Women with partially blocked fallopian tubes but who still have one functional tube may be candidates for ZIFT. It ensures that fertilized eggs are implanted in the fallopian tubes, which is beneficial for embryo development.
Previous IVF Failure:
For couples who have undergone IVF previously without success, especially when embryos fail to implant, ZIFT may be considered as a secondary treatment option.
After undergoing ZIFT, women may experience the following common post-procedure symptoms:
Mild Cramping:
Mild cramping is normal following ZIFT, as the uterus adjusts to the embryo implantation process.
Spotting or Light Bleeding:
Light spotting or bleeding may occur after ZIFT, particularly in the days following embryo transfer. This is common and typically resolves within a few days.
Pregnancy Symptoms:
If the procedure is successful, typical pregnancy symptoms such as nausea, fatigue, and breast tenderness may appear.
The need for ZIFT is typically identified after a thorough fertility evaluation, which includes tests to assess the cause of infertility and determine whether ZIFT is a suitable treatment option. Here’s how the diagnosis process typically works:
Ovulation and Hormonal Testing:
Blood tests for FSH, LH, and estrogen levels help determine the woman’s ovarian reserve and ovulatory function. Ultrasound scans are used to assess the health of the ovaries and the presence of follicles.
Hysterosalpingography (HSG):
A HSG is used to assess the condition of the fallopian tubes. The procedure involves injecting dye into the uterus and fallopian tubes and taking X-ray images to check for blockages or abnormalities in the tubes.
Semen Analysis:
A semen analysis is conducted to evaluate sperm count, motility, and morphology. Sperm issues may lead to the recommendation of ZIFT after IVF.
Ovarian Reserve Testing:
Tests such as AMH (Anti-Müllerian Hormone) levels and FSH tests are used to assess the quality and quantity of a woman’s eggs, guiding whether IVF or ZIFT is the best option.
Genetic Testing:
In some cases, genetic testing is recommended to check for potential inherited conditions that might affect the success of implantation or the health of the embryo.
ZIFT is an advanced fertility treatment that involves a combination of egg retrieval, fertilization, and embryo transfer into the fallopian tubes. The procedure includes the following steps:
The first step involves ovarian stimulation, where the woman is given hormonal medications (such as FSH and LH) to produce multiple eggs. Once the eggs are mature, they are retrieved through a minor procedure known as egg aspiration.
The eggs are fertilized with sperm (from the partner or a donor) in the lab using traditional IVF or ICSI. The fertilized egg becomes a zygote.
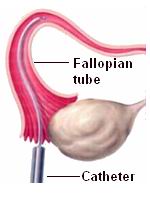
After fertilization, the zygote (fertilized egg) is placed directly into one of the fallopian tubes using a catheter. This is the defining step of ZIFT, as it differs from traditional IVF, where the zygote is implanted in the uterus.
About 10-12 days after the procedure, a blood test is performed to check for hCG levels to confirm pregnancy. If the test is positive, an ultrasound is conducted after a few weeks to confirm fetal development.
While ZIFT has high success rates, there are steps that can be taken to manage and increase the likelihood of a successful outcome.
Genetic Screening:
Pre-implantation genetic testing (PGT) can help screen embryos for genetic abnormalities before transfer, reducing the risk of miscarriage or genetic disorders.
Healthy Lifestyle Choices:
Women should focus on maintaining a healthy lifestyle by eating a balanced diet, exercising regularly, avoiding smoking, and limiting alcohol consumption to improve fertility and increase the chances of success with ZIFT.
Hormonal Management:
Proper management of hormonal levels before and after the procedure is essential for embryo development and implantation.
Close Monitoring:
Throughout the process, including ovarian stimulation, egg retrieval, fertilization, and embryo transfer, the woman will be closely monitored with ultrasound scans and blood tests to track progress.
Post-Transfer Care:
After the zygote is transferred to the fallopian tubes, the woman should avoid heavy physical activity and rest as much as possible to ensure the best chances of embryo implantation.
While ZIFT is a generally safe procedure, like all medical treatments, it carries some risks and potential complications.
Ovarian Hyperstimulation Syndrome (OHSS):
OHSS is a condition where the ovaries over-respond to stimulation and become swollen. Symptoms include abdominal pain, bloating, and fluid retention. This can be managed with proper monitoring and care.
Multiple Pregnancies:
Although only one or two embryos are typically transferred, multiple pregnancies (twins or triplets) can occur, leading to preterm birth, low birth weight, and increased medical risks.
Ectopic Pregnancy:
There is a small risk of the embryo implanting outside the uterus, usually in the fallopian tubes, which can lead to an ectopic pregnancy. This requires medical intervention.
Infection or Bleeding:
As with any surgical procedure, there is a slight risk of infection or bleeding at the egg retrieval or embryo transfer sites.
Undergoing ZIFT can be an emotionally taxing process for both the woman and the couple. The journey of infertility treatments requires resilience and support.
Emotional Health:
ZIFT, like all ART procedures, can bring about feelings of stress, hope, and uncertainty. It’s important to maintain emotional support through counseling and support networks.
Physical Recovery:
After the procedure, women may experience mild discomfort, cramping, or spotting, which usually resolves within a few days.
Health and Wellness:
Women should focus on staying physically healthy through proper nutrition, exercise, and stress management to improve the chances of success.
Communication and Support:
Couples should maintain open communication throughout the process and support each other emotionally. Working together as a team during the fertility journey can strengthen the bond between partners.
Zygote Intra-Fallopian Transfer (ZIFT) is a form of assisted reproductive technology (ART) in which a fertilized egg (zygote) is placed directly into the fallopian tube. Unlike in vitro fertilization (IVF), where the embryo is transferred to the uterus, ZIFT involves placing the zygote in the fallopian tube to allow natural implantation to occur.
The main difference between ZIFT and IVF is where the embryo is placed:
IVF: The fertilized embryo (which has developed for several days) is transferred into the uterus.
ZIFT: The fertilized egg (zygote) is placed directly into the fallopian tube, typically within 24 hours of fertilization, before it has developed into a multi-cell embryo.
ZIFT is considered a hybrid technique that combines aspects of both IVF and gamete intra-fallopian transfer (GIFT).
ZIFT may be recommended for women who:
Have healthy fallopian tubes and can potentially allow for the natural process of embryo implantation.
Have had previous IVF cycles that failed to result in pregnancy, especially if uterine issues were suspected.
Prefer a technique that mimics natural fertilization by allowing the fertilized egg to travel
down the fallopian tube and implant in the uterus naturally.
However, ZIFT is not suitable for all patients, and it is only recommended when there is a
good chance of successful fertilization and tube function.
ZIFT involves the following steps:
Ovarian stimulation: The woman is given hormones to stimulate her ovaries to produce multiple eggs.
Egg retrieval: Once the eggs are mature, they are retrieved using a needle under light sedation.
Fertilization: The eggs are fertilized in the laboratory with sperm from the partner or donor, and the resulting zygotes are cultured.
Zygote transfer: Within 24 hours of fertilization, the zygotes (early embryos) are placed into the fallopian tube using a thin catheter.
The success rates of ZIFT are generally similar to IVF, but they depend on factors like the woman's age, the health of the fallopian tubes, and the quality of the eggs and sperm. Success rates for ZIFT range from 20% to 40% per cycle, with higher chances of success if the fallopian tubes are healthy and if the woman is younger. ZIFT is often used when previous IVF cycles have failed due to problems with embryo implantation.
The potential advantages of ZIFT include:
Mimicking natural fertilization: By transferring the zygote into the fallopian tube, ZIFT allows the embryo to travel naturally to the uterus, which may increase the chances of successful implantation.
Higher success in women with healthy fallopian tubes: ZIFT may be more successful in women whose fallopian tubes are open and functional, offering a more natural approach to fertilization and embryo transfer.
Possibly better implantation rates: Since the zygote is placed directly into the fallopian tube, it may have a better chance of implantation compared to when it is transferred to the uterus in IVF.
The risks of ZIFT are similar to those of IVF and other assisted reproductive technologies, and they include:
Ovarian hyperstimulation syndrome (OHSS): A condition where the ovaries become swollen and painful due to overstimulation from fertility drugs.
Multiple pregnancies: If more than one zygote is transferred, there is a risk of twins or more, which can carry risks for both the mother and babies.
Ectopic pregnancy: There is a small risk that the zygote may implant outside the uterus, such as in the fallopian tube.
Infection or bleeding: As with any surgical procedure, there is a risk of infection or bleeding from the egg retrieval procedure or the zygote transfer.
The ZIFT procedure typically takes about 3-4 weeks. This includes the time for ovarian stimulation, egg retrieval, fertilization, and the zygote transfer. After the zygote transfer, patients typically wait 10-14 days before taking a pregnancy test to confirm whether implantation was successful.
If ZIFT is unsuccessful, the couple may consider:
Reattempting ZIFT: With adjustments such as modifying the ovarian stimulation protocol or using frozen embryos from a previous cycle.
Switching to IVF: If ZIFT fails, IVF may be considered as an alternative
option, especially if there are concerns about the function of the fallopian tubes.
The fertility specialist will discuss the next steps and offer guidance based on the
individual’s specific situation.
ZIFT is not suitable for everyone. It is typically recommended for:
Women with healthy fallopian tubes who are able to naturally allow the embryo to implant.
Women who have had a failed IVF cycle and are seeking a method that may improve implantation
success.
However, it is not suitable for women who have blocked or damaged fallopian tubes, as the
zygote must pass through the tube for implantation. In these cases, IVF is usually
recommended instead.

Few Major Hospitals for IVF are:
Thailand, Malaysia, Singapore, Turkey and India are the most cost effective locations that offer up to almost 80% savings in comparison to the US.
SurgeryPlanet facilitates a plethora of services to the medical treatment traveler also which includes, a hassle free and discounted travel option, a welcome hand at the airport on arrival, travel in an air-conditioned car, round the clock service & support. Your medical evaluation is pre arranged with the least of waiting time. Once your assessment is complete and found medically fit, the procedure is immediately scheduled without a waiting period. Please read through our Services and Testimonials to understand and select your best options.
Major Treatments Abroad: Obesity / Bariatric Surgery | Spine Surgery | Stem Cell therapy | Fertility treatment | Knee replacement in India and Thailand | Heart Surgery | Organ transplant | Ayurveda Treatment | Heart valve replacement | Hip resurfacing | Hospitals in India and Thailand for Laparoscopic Sterilization| Best hospitals in Asia | JCI & ISO certified Hospitals | Cost effective medical procedures | Healthcare tourism | Complete privacy for affordable cost | Weight loss procedures | Infertility treatment | Board certified physicians | Low cost surgeries
SurgeryPlanet is an Healthcare Facilitator and not a Medical service provider. The information provided in this website is not to be used for diagnosis or treatment of any medical condition or use for any medical purposes. We provide information solely for medical travel facilitation and do not endorse any particular health care provider, hospital, facility, destination or any healthcare service or treatment listed. We are not an agent for, or affiliated to any health care provider, or service listed in our website and is not responsible for health care services provided by them. Choice of hospital or doctor for your healthcare services is your independent decision. Consult your domestic licensed health care provider before seeking the services of any health care provider you learn about from our website.

